 Much is being made of palliative care these days, especially in the doctor-assisted suicide debate. Prominent palliative care specialists such as Ira Byock and former assisted-suicide advocate Diane Meier strongly oppose such legislation in our new era of palliative care.
Much is being made of palliative care these days, especially in the doctor-assisted suicide debate. Prominent palliative care specialists such as Ira Byock and former assisted-suicide advocate Diane Meier strongly oppose such legislation in our new era of palliative care.
According to the Center to Advance Palliative Care (CAPC), headed by Dr. Meier, palliative care “is specialized medical care for people living with serious illness. It focuses on providing relief from the symptoms and stress of a serious illness,” and “is appropriate at any age and at any stage in a serious illness and can be provided along with curative treatment.”
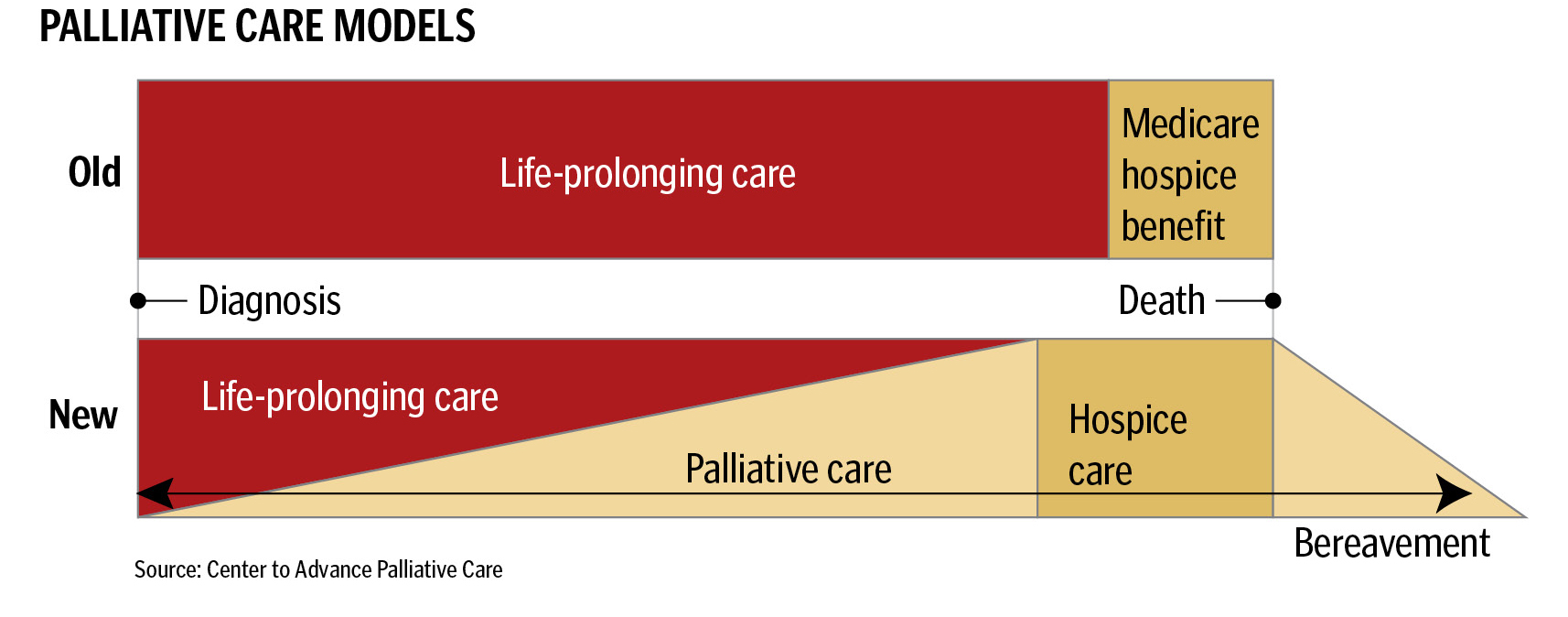
Palliative care is not hospice, as anyone in the field would tell you. Here is a graphic from CAPC demonstrating the “old” and “new” models of care:
My step-father, Dick, had congestive heart failure, stage IV renal cancer in his lungs, and required dialysis. His appetitie and sleep were poor and he had bouts of breathing difficulties, much of which was due to untreated clinical anxiety. But he still cared for himself, drove himself to dialysis, and received chemotherapy. My mother had difficulty coordinating the different instructions from the nephrologist, oncologist, and cardiologist, which sometimes conflicted, none of whom addressed his symptoms. I told her to ask about palliative care for him, since he was the perfect patient for such services based. She received a resounding, “No,” from all the doctors.
This reaction truly confused me until I learned that under Medicare palliative care services are paid through hospice benefits. In other words, Dick needed to go on hospice in order to receive palliative care. Signing on to hospice means giving up all other treatments, the so-called “life-prolonging care” in the models above. Without dialysis, Dick would die in a matter of days, so hospice was out of the question.
That “old” model of palliative care is not so old. That makes the push for palliative care in reality a push to surrender life-sustaining treatments. Beware of former assisted-suicide advocates turned palliative-care-specialists and the false hope they present.

